


 among Egyptian Geriatric patients: a multi-center cross-sectional study | BMC Oral Health")
Study design, settings, and participants
In this cross-sectional study, a random sample of 400 Egyptian geriatric patients aged over 60 years, frequently visited four different dental centers as an outpatient clinic, the periodontology department of Ain Shams University, Cairo Governorate, and the research centers of the Ministry of Health and Population, MOHP. The Dentists Training Center in Mansoura, Dakahlia Governorate. The Dentists Training Center in Damnhour, Beheira Governorate. The Specialized Dental Center in Port Said, Port Said Governorate. These centers were chosen based on their high geriatric patient flow and geographic distribution to capture diverse socioeconomic and health backgrounds. A random sampling technique was used within these centers to ensure that participants were not selectively chosen based on their oral health status, increasing the study’s generalizability. Conducted in a single visit, thereby eliminating the need for follow-up assessments. Importantly, this specific dental clinic houses a removable dental laboratory, such a facility attracts a high flow of geriatric patients, who are the primary focus of our study, As a result, the sample although not fully representative of the general Egyptian elderly population, is still relevant to the study objective, as it captures a population segment closely aligned with the study focus on geriatric oral health and the impact on oral health-related quality of life. Inclusion/Exclusion Criteria: Inclusion: both genders, male and female patients aged ≥ 60 years diagnosed with periodontitis and willing to participate. Exclusion: Individuals with < 2 remaining teeth, severe cognitive impairments, or severe systemic diseases that might interfere with oral health assessment, direct socioeconomic exclusion criteria were not applied. The research adhered to established ethical guidelines, and the study was approved by the Faculty of Dentistry Ain Shams University Research Ethics Committee (FDASU-REC) with approval number (FDASU-REC IM052302) and the research ethical committee of the Egyptian Ministry of Health and Population, MOHP with approval number (12–2023/16). A participant’s confidentiality was protected, and their data were fully secured following ethical guidelines.
Written informed consent was signed by all participants prior to the clinical examination. In the case of illiterate patients, the consent form was read aloud to the participants. Their full understanding of the study details was ensured, and verbal consent was obtained in the presence of a witness, who then signed the consent form on behalf of the participant. Alternatively, the participants could provide consent by placing a thumbprint on the consent form.
Questionnaire
All the participants answered a structured questionnaire before the clinical examination, The questionnaire contained items concerning a sociodemographic background, educational level, smoking habits, medical conditions, medication use, frequency of dental visits, and their regularity, and patterns of teeth brushing. Education levels were assessed by six alternative responses due to the variation in educational levels across the Egyptian population: “illiterate”, “primary”, “preparatory”, secondary”, and “university”. Additionally, smoking habits were assessed by three alternative responses: never smoker”, former smoker, and current smoker. The “Current smoker” was defined as an individual who smoked at least one cigarette daily. Current smokers also reported the number of cigarettes consumed daily. The oral health-related quality of life (OHRQOL) was assessed via the oral health impact profile (OHIP-14) [19, 20]. The questionnaire consists of 14 items divided into seven dimensions: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap.
Ratings are made on a 5-point Likert scale for each item: 0 = never, 1 = hardly ever, 2 = occasionally,
3 = fairly often, and 4 = very often, with the sum of the scores ranging from 0–56. Higher OHIP-14 scores indicate poorer OHRQOL. Participants reporting a negative impact (response codes: 3’fairly often’ and 4’very often’) on one or more of the 14 items were categorized as having a negative impact on OHRQOL, whereas those who had response codes ranging from 0–2 for all items were considered to have fair OHRQOL by the OHIP-14. Language and Cross-Cultural Adaptation of OHIP-14: The OHIP-14 questionnaire was used in Modern Standard Arabic, the primary language of participants. It has been previously validated for use in Arabic-speaking populations. No major cultural adaptations were needed, as the questionnaire’s constructs align with standard oral health assessment metrics [21, 22].
Clinical examinations
Two calibrated periodontists conducted clinical examinations. Inter-examiner reliability was tested using Cohen’s kappa (κ = 0.86), indicating high agreement. The clinical examination was divided into three segments the 1 st segment included recording the prosthesis if available as a removable partial or complete denture, and was fixed as a crown, bridge, or implants; the 2nd segment included registration of the DMF, and the total number of permanent teeth filled, missing, and decaying. Every tooth, excluding the third molars, was included [23, 24]. The 3rd segment included the recording of periodontal parameters such as tooth mobility, periodontal probing pocket depth (PPD), clinical attachment level (CAL), bleeding on probing (BOP), and the plaque index (PI). All periodontal parameters were recorded and written on periodontal charts [25].
Periodontal status was assessed based on the consensus report from the 2017 World Workshop on the Classification of Periodontal and Peri-implant Diseases and Conditions (2018 EFP/AAP classification) [26]. Plaque index (PI): Supragingival plaque presence was recorded on four tooth surfaces using this index. Plaque was documented as present (+) or absent (−), and the plaque incidence was calculated as a percentage [26]. Gingivitis Index (Bleeding on Probing (BOP): Gingival bleeding was assessed on all tooth surfaces, with bleeding recorded as either present (+) or absent (-). Gingivitis severity was expressed as a percentage [27, 28]. Clinical Attachment Loss (CAL): Indicates junctional epithelium migration and connective tissue loss, key in periodontitis assessment. Measured from the cementoenamel junction (CEJ) to the periodontal pocket base. CAL Calculations: Gingival margin at CEJ → CAL = PD, Coronal to CEJ → CAL = PD – GML, Apical to CEJ → CAL = PD + GML. CAL was recorded as a means of patient periodontal status. Periodontal Pocket Depth: Using a calibrated probe, measure six sites per tooth to assess periodontal health, PPD recorded as the mean of the patient’s status. Periodontal health was comprehensively assessed by measuring probing depths and clinical attachment loss (CAL) at six sites per tooth. These individual measurements were summed to calculate the total probing depth and total CAL for each patient. The mean values were then determined by dividing these totals by the number of sites measured [29, 30]. Periodontitis is divided into four stages based on clinical attachment loss (CAL), bone loss, and probing pocket depth (PPD). Stage I has CAL of 1–2 mm and bone loss under 15%. Stage II shows CAL of 3–4 mm and bone loss of 15–33%. Stage III and IV involve CAL of 5 mm or more, bone loss to the middle root, and PPD of 6 mm or more, with Stage IV requiring complex treatment due to the loss of five or more teeth [31].
Variables
Outcome (Dependent Variable): The primary focus of this study is the impact on Oral Health-Related Quality of Life (OHRQOL).
Main Exposure Variables (Key Predictors of OHRQOL): Periodontitis is assessed through periodontal parameters, including probing pocket depth (PPD), clinical attachment loss (CAL), and bleeding on probing (BOP).
Mediators (Pathways through which exposures affect OHRQOL): The Decayed, Missing, and Filled Teeth (DMF) index acts as a mediator, influencing the functional and aesthetic dimensions of quality of life. Additionally, the presence of dental prostheses affects functional capacity, aesthetic considerations, and adaptation to missing teeth.
Confounders (Factors influencing both exposure and outcome, potentially biasing the effect estimate): Age serves as a significant confounder, impacting both periodontal health and OHRQOL. Gender affects health behaviors and perceptions of quality of life, while educational level influences awareness of oral hygiene and access to dental care. Medical conditions such as diabetes and cardiovascular diseases also affect periodontal health and overall well-being. Smoking is a strong confounder, affecting both periodontal and systemic health.
Colliders (Variables influenced by two or more other variables, introducing potential bias if adjusted for improperly): Variables such as tooth brushing and dental visits are influenced by education level and affect plaque presence and periodontal status. These variables must be carefully considered to avoid introducing bias in the analysis (Fig. 1).

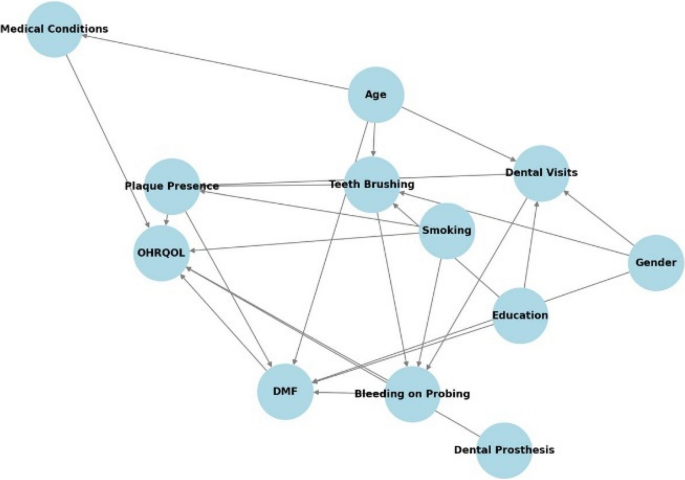
Directed Acyclic Graph (DAG) representing the relationships among periodontitis risk factors and OHRQOL
Study size and statistical analyses
The sample size was determined using G*Power software based on previous epidemiological data on periodontitis prevalence in geriatric populations (effect size = 0.3, power = 80%, α = 0.05). A random sampling approach was used within each center to minimize selection bias. Assuming a confidence limit of 5% and a confidence level of 95%, the minimum required sample size was 345 elderly patients. An additional 10% was added to compensate for potential losses, resulting in a total sample size of 400 cases after rounding. The collected data were analyzed using SPSS (Statistical Package for the Social Sciences), version 22. Quantitative data were tested for normality using the Kolmogorov‒Smirnov test and were then described as means and standard deviations for normally distributed data, and as medians and ranges for non-normally distributed data. Qualitative data were presented as numbers and percentages. The Chi-square test was used to examine associations between categorical variables (e.g., gender, age, education level) and their relationship with oral health-related quality of life (OHRQL). The Chi-square test also used to assess the stage of periodontitis in relation to oral health-related quality of life (OHRQOL). Logistic regression analysis was employed to evaluate the association between periodontitis severity and OHRQOL impairment, adjusting for potential confounders such as age, gender, and smoking habits. The results of the regression analyses were presented as odds ratios (ORs) with 95% confidence intervals (CIs). The level of significance was set at p < 0.05. The Kolmogorov–Smirnov test was used to assess normality prior to applying statistical tests.
link